Somewhere between your third and fourth session of the day, you realize your last progress note barely mentioned the goal you’ve been working on for two months. The session was good, and the work was real, but the note reads like a summary of what happened, not evidence of where treatment is going. If that sounds familiar, GIRP notes might be the format that fixes it.
GIRP notes are a goal-anchored progress note format that keeps every session tied directly to what a client is working toward. They’re especially useful in managed care, community mental health, and any setting where demonstrating treatment progress isn’t optional; it’s a billing requirement. This guide covers the format, a full clinical example, common pitfalls, and how AI is changing the documentation picture.
Table of Contents
- What Are GIRP Notes?
- Why Use GIRP Notes?
- GIRP Note Format Breakdown
- GIRP Note Example (Full Clinical Scenario)
- GIRP vs. BIRP vs. SOAP vs. DAP: Comparison Guide
- Common Mistakes in GIRP Notes
- How AI Can Write Your GIRP Notes
- Frequently Asked Questions
- References
1. What Are GIRP Notes?
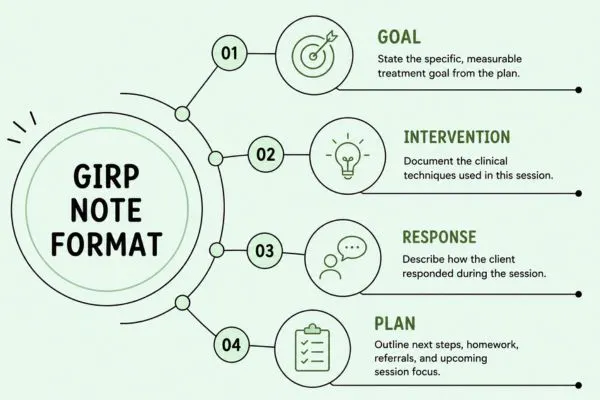
GIRP stands for Goal, Intervention, Response, and Plan. It is a structured progress note format used in outpatient therapy, community mental health, substance use treatment, and case management settings. Unlike SOAP or DAP notes, GIRP notes lead with the client’s treatment goal, which means every session is documented in direct relation to what the client is actively working toward.
- Goal: The specific treatment plan goal being addressed in this session.
- Intervention: The clinical techniques and therapeutic approaches used by the clinician.
- Response: How the client responded — behaviorally, emotionally, and cognitively — to the interventions.
- Plan: Next steps: homework, next session focus, referrals, or adjustments to the treatment approach.
The goal-first structure is what sets GIRP apart. It creates a documentation thread that connects your treatment plan to your session notes, which is exactly what payers and auditors are looking for when they review records.
2. Why Use GIRP Notes?
They make medical necessity easier to demonstrate. Managed care payers require documentation showing that treatment is clinically justified and progressing toward defined outcomes. Because every GIRP note starts with a treatment plan goal, medical necessity is built into the structure. You’re not trying to retroactively connect a session to a goal; it’s the first thing in the note.
They keep treatment plan-focused. Treatment drift happens. Sessions wander. GIRP notes create a natural checkpoint: before you write the note, you’re identifying which goal was addressed. That practice keeps sessions anchored to the client’s stated objectives.
They support continuity of care. When multiple providers are involved, or when a client’s chart is reviewed by a supervisor, billing team, or licensing board, GIRP notes make the treatment arc visible. A reviewer can trace exactly which goals were addressed, how, and with what result across any number of sessions.
They reduce audit risk. Vague progress notes are the most common trigger for payer audit findings. GIRP’s structure pushes against vagueness by requiring specific goal references, intervention descriptions, and documented client responses.
3. GIRP Note Format Breakdown
G — Goal
State the treatment plan goal being addressed in this session. Copy it directly from the treatment plan where possible, or reference it clearly enough that the connection is unambiguous.
- "Client will develop three evidence-based coping skills for managing depressive symptoms within 60 days."
- "Client will reduce frequency of panic attacks to no more than one per week within 90 days as measured by self-report."
- "Client will demonstrate improved conflict communication skills within couples sessions over the next 8 weeks."
Key rule: The Goal section is not a description of the session topic. It is the specific, measurable objective from the treatment plan. If your treatment plan goals are vague, GIRP notes will expose that quickly, which is actually a useful feedback mechanism.
I — Intervention
Document the specific clinical techniques applied during the session. Name the technique, the modality, and how it was used in this particular session.
- "Therapist utilized CBT to review a thought record completed between sessions and identify three automatic negative thoughts related to self-worth."
- "Motivational interviewing techniques were used to explore ambivalence around medication adherence and identify internal motivators for change."
- "Exposure hierarchy was reviewed; client completed two low-level imaginal exposure exercises targeting social anxiety scenarios."
- "Psychoeducation was provided on the relationship between avoidance behavior and the maintenance of anxiety symptoms."
Avoid: "Therapy was provided." Better: "Therapist guided client through a values clarification exercise using ACT principles to identify discrepancies between current avoidance behavior and stated life priorities."
R — Response
Describe how the client actually responded to what you did. This section shows the therapeutic relationship in action and documents treatment effectiveness.
- "Client arrived with completed thought record and engaged actively in collaborative review throughout the session."
- "Client initially expressed frustration when discussing medication but demonstrated increasing openness as session progressed."
- "Client reported anxiety reduced from 8/10 to 4/10 following exposure exercise; appeared visibly calmer by end of session."
The Response section is the one most frequently underwritten, and the one most often scrutinized in audits. It provides clinical evidence that something happened in the session, not just that you were present. Document resistance, engagement level, emotional shifts, and any notable in-session moments.
P — Plan
Close with a clear record of next steps.
- Homework or between-session assignments
- Focus areas and goals for the next session
- Referrals made or pending (psychiatry, primary care, support groups)
- Any changes to treatment frequency, modality, or plan objectives
- Crisis safety planning if applicable
- Scheduled appointment date
4. GIRP Note Example (Full Clinical Scenario)
Client Presentation: Major Depressive Disorder, recurrent episode, Session 6
GOAL
Client will identify and challenge negative automatic thoughts related to self-worth, working toward the treatment goal of reducing depressive symptoms by 50% within 90 days as measured by PHQ-9 scores.
INTERVENTION
Therapist utilized CBT to review a thought record completed between sessions. Collaborative discussion helped the client identify three automatic negative thoughts related to personal failure and social withdrawal. Socratic questioning was used to evaluate evidence for and against each belief. Behavioral activation planning was introduced; client identified two enjoyable activities to schedule this week and selected specific times for each.
RESPONSE
Client arrived with completed thought record and engaged actively throughout the review process. By end of session, client independently identified “all-or-nothing thinking” as a pattern across multiple thought entries. Expressed optimism about behavioral activation plan, stating it felt “manageable.” PHQ-9 administered at session end: score 14 (down from 18 at last session). Client denied suicidal ideation.
PLAN
Client will complete two behavioral activation activities before next session and record outcomes in mood journal. Next session will continue CBT thought record practice and introduce problem-solving techniques for work-related stressors. PHQ-9 to be re-administered at session 8. Next appointment scheduled in one week. Therapist to follow up on any barriers to behavioral activation at session start.
5. GIRP vs. BIRP vs. SOAP vs. DAP: Comparison Guide
Format choice usually comes down to three factors: your practice setting, your payer’s requirements, and what information you most need to track. Here’s how the common formats compare:
Format | Best For | Strength | Limitation |
|---|---|---|---|
GIRP | Goal-driven outpatient therapy, managed care | Directly ties each session to treatment plan goals | Can feel formulaic if goals are poorly written |
BIRP | Behavioral health, response-focused documentation | Captures client response to interventions clearly | Less emphasis on goal tracking across sessions |
SOAP | Medical/integrated care, multi-disciplinary teams | Universally recognized across clinical disciplines | Subjective/Objective split can feel redundant in talk therapy |
DAP | Individual outpatient therapy, fast documentation | Concise and quick to write | Less granular on intervention specifics |
When to choose GIRP: You’re in a setting where treatment plan compliance is closely monitored, managed care, community mental health, or intensive outpatient. Your notes will be reviewed by utilization management teams. You want documentation that naturally demonstrates progress toward stated goals over time.
6. Common Mistakes in GIRP Notes
- Stating a session topic instead of a treatment plan goal. "Client discussed anxiety" is not a goal. "Client will reduce anxiety symptoms to sub-clinical levels within 90 days as measured by GAD-7" is. If your Goal section sounds like a session summary, rewrite it.
- Vague intervention language. "Therapist used CBT" is not sufficient. Name the specific technique and describe how it was applied in this session. "Therapist utilized cognitive restructuring to help client examine evidence for catastrophic predictions about a job interview" tells the whole clinical story.
- Skipping the Response section. This is the most common omission, and the most costly in an audit. If a client resisted, document the resistance and your clinical response to it. Engagement, affect changes, and insight shifts all belong here.
- Recycling the same Plan language across sessions. "Continue current treatment" is not a plan. Specify what will be covered, what homework was assigned, and when the next appointment is. If the plan genuinely hasn’t changed, document why.
- Disconnected goals. If the goal in your note doesn’t match a goal on the current treatment plan, that’s a documentation discrepancy. Payers will flag it. Keep notes and treatment plans synchronized.
- Late documentation. Writing notes two or three days after a session increases the risk of inaccurate detail. Best practice is same-day or next-day documentation. If there’s a delay, note the date of documentation separately from the session date.
7. How AI Can Write Your GIRP Notes
If you’re seeing 20+ clients a week, GIRP notes, even well-written ones, add up fast. Each note takes 10–20 minutes when written from scratch. That’s 3–7 hours of documentation every week, most of it after hours.
AI-assisted documentation platforms like Supanote are built specifically for this problem. After a session, you give Supanote a verbal summary describing the goal addressed, what you did, and how the client responded, and the AI generates a structured GIRP note in under a minute. You review, edit, and finalize. Most therapists cut documentation time by 60–70%.
What AI handles well:
- Structuring your verbal summary into clean G/I/R/P sections
- Applying clinical language consistently across all notes
- Maintaining note format alignment with your treatment plan goals
- Flagging underdeveloped sections before you finalize
- Supporting multiple formats: GIRP, BIRP, SOAP, DAP at the click of a button
Where you still own the work:
- AI works from what you give it. A vague verbal summary produces a vague note. Be specific about which goal you addressed and what the client actually did.
- Risk documentation requires your clinical judgment. AI will prompt you for safety information, but you make the call.
- Nonverbal cues, the quality of silence, relational dynamics these live in the room, not in a transcript. Your clinical read belongs in the note after you’ve reviewed the AI draft.
Supanote is HIPAA-compliant, provides a signed BAA for every account, and supports GIRP, BIRP, SOAP, DAP, PIRP, and custom formats. The free plan lets you generate notes immediately; no credit card required.
Try Supanote Free — Cut Note-Writing Time by 70% →
Frequently Asked Questions
1. What makes GIRP notes different from SOAP or DAP notes?
SOAP and DAP notes document what happened in a session, what the client reported, what you observed, what you did, and what’s next. GIRP notes lead with the treatment plan goal, which reframes the entire note around where treatment is headed rather than just what occurred. This makes GIRP especially valuable in goal-monitored settings where payers want documentation of progress toward specific objectives, not just a session summary.
2. Are GIRP notes accepted by insurance companies?
Yes, in most cases. GIRP notes satisfy the core requirements insurance payers look for: documented presenting concerns (Goal), clinical treatment (Intervention), treatment response (Response), and ongoing care plan (Plan). As with any format, the content matters more than the acronym. Vague GIRP notes will fail a utilization review just as vague SOAP notes will. The structure just makes it easier to write notes that are inherently compliance-friendly.
3. Can I use GIRP notes for group therapy?
Yes, with individualization. In group settings, the Goal section documents which treatment plan goal is being addressed for this specific client within the group context. The Intervention section describes both the group modality and any individualized therapeutic moves you made with this client. The Response section captures how this client engaged with group process, peers, and facilitation. Many practices write a shared Intervention section and individualize the G, R, and P per group member.
4. How long should a GIRP note be?
For standard outpatient sessions, a complete GIRP note typically runs 150–300 words. Longer isn’t better; specific is better. A tight 180-word note that covers all four sections with precise clinical language is more defensible than a padded 400-word note full of generalities. Budget your words for the Response section, which is where most notes fall short.
5. Do telehealth sessions require different GIRP notes?
The clinical content doesn’t change, but you should add documentation of the session modality (e.g., "Session conducted via HIPAA-compliant video platform"), confirmation that the client was located in the state where you’re licensed, and a note that the client provided telehealth consent. Some payers also require a telehealth modifier on the corresponding CPT billing code. Check with your specific payers.
6. What if a session addresses more than one treatment goal?
You have two options. Some clinicians write a separate GIRP note for each goal addressed, which creates maximum clarity. Others write a single note and list multiple goals in the Goal section, noting which interventions related to which goal. Either approach is defensible; just be consistent within your practice and make sure each goal-intervention pairing is clear to any reader.
7. Can supervisees and interns write GIRP notes?
Yes, pending state-specific supervision requirements. Supervisees can author and sign progress notes in most states, with the supervising clinician co-signing. Your supervision agreement and informed consent documents should specify that notes are reviewed and co-signed by a licensed supervisor. Document supervision sessions where note review occurs, this creates a clear audit trail if records are ever scrutinized.
8. What should I do if a client declines to work on their treatment plan goals in session?
Document it honestly. The Goal section still names the goal that was the intended focus. The Response section is where you capture the client’s resistance, your clinical response to it, and any insight or shift that followed. For example: "Client declined to engage with scheduled thought record exercise, expressing hopelessness about the utility of CBT techniques. Therapist explored ambivalence; client agreed to discuss one recent situation where a coping attempt was partially successful." This shows active clinical work, not avoidance on your part.
9. How do GIRP notes hold up in a licensing board review?
Well-structured GIRP notes are strong evidence of intentional, goal-directed treatment. The format makes it easy to show that each session was connected to a treatment plan, that specific clinical techniques were applied, and that client progress was monitored. The risk areas are the same as any format: vague language, copy-pasted notes, underdeveloped Response sections, or goals that don’t match the current treatment plan. Consistent, specific GIRP documentation works in your favor.
10. Is there AI software that writes GIRP notes automatically?
Yes. Purpose-built mental health documentation tools like Supanote generate GIRP-formatted notes from a post-session verbal summary or recording. The AI produces a structured first draft; you review and finalize. Supanote is HIPAA-compliant, supports GIRP, BIRP, SOAP, DAP, and PIRP formats, and is built specifically for mental health providers in private practice and group clinic settings.
References
American Psychological Association. (2023). Ethical principles of psychologists and code of conduct. https://www.apa.org/ethics/code
U.S. Department of Health & Human Services. (2024). HIPAA for professionals. https://www.hhs.gov/hipaa/for-professionals
Kroenke, K., & Spitzer, R. L. (2002). The PHQ-9: A new depression diagnostic and severity measure. Psychiatric Annals, 32(9), 509–515.
Wiger, D. E. (2012). The psychotherapy documentation primer (3rd ed.). John Wiley & Sons.
Zur Institute. (2023). Psychotherapy notes and progress notes: Legal, ethical, and clinical issues. https://www.zurinstitute.com/resources/psychotherapy-notes/
