A new client books for next Tuesday. Between now and then, you need their history, their presenting concern, their meds, their risk profile, their insurance, and a signed consent, and on Tuesday you’d like to start the actual work instead of spending the first twenty minutes transcribing a paper form into your chart. Multiply that by every new client, and intake quietly becomes one of the biggest admin drains in a practice.
This guide covers how AI is changing client intake for mental health practices, gives you a complete copy-paste intake form template you can use today, walks through what each section should capture and why, and is honest about where AI genuinely helps versus where a clinician still has to make the call. There’s also a compliance section, because intake forms collect some of the most sensitive PHI you’ll ever hold.
What “AI Intake” Actually Means
“AI intake” gets used loosely, so here’s the practical breakdown of what AI can do at the intake stage:
- Smart intake forms — digital forms clients complete before the first session, with logic that adapts questions based on answers (e.g., expanding the substance-use section only if relevant).
- Summarizing intake responses — turning a long completed form into a concise clinical summary you can read in a minute before the session.
- Drafting the intake/biopsychosocial assessment — generating the structured intake note from the first session, the same way AI drafts progress notes.
- Reducing double entry — pushing intake data into your EHR instead of you re-typing it.
What AI does not do is decide clinical significance, whether a reported symptom warrants a risk assessment, whether a history detail changes your formulation. That’s yours. AI organizes and drafts; you interpret.
A Complete Client Intake Form Template (Copy-Paste)
Here’s a comprehensive intake form template for a mental health practice. Adapt sections to your specialty, and have clients complete it before the first session.
CLIENT INTAKE FORM
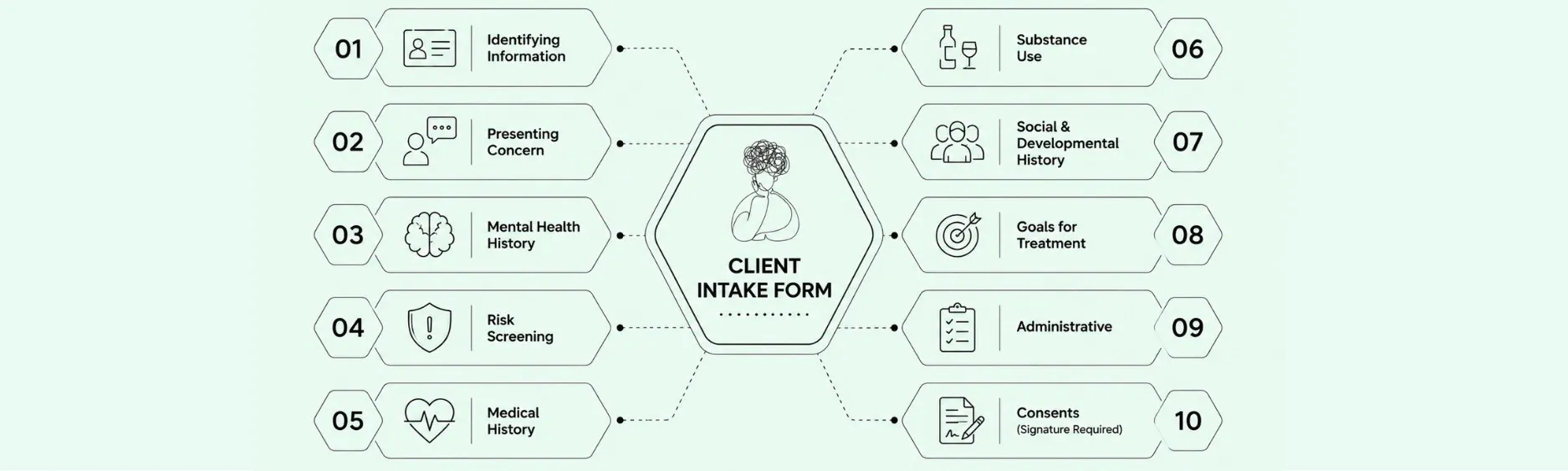
1. Identifying Information Full name · Preferred name/pronouns · Date of birth · Address · Phone · Email · Emergency contact (name, relationship, phone)
2. Presenting Concern What brings you in at this time? · When did it start? · How is it affecting your daily life (work, relationships, sleep, appetite)? · What have you tried so far?
3. Mental Health History Previous therapy or counseling (when, with whom, helpful or not) · Previous psychiatric hospitalizations · Current and past mental health diagnoses · Family history of mental health conditions
4. Risk Screening Current or past thoughts of harming yourself? · Current or past thoughts of harming others? · History of self-harm? · (This section flags items for clinical follow-up, it does not replace a clinical risk assessment.)
5. Medical History Current medical conditions · Current medications (name, dose, prescriber) · Allergies · Primary care provider · Relevant surgeries/hospitalizations
6. Substance Use Alcohol (frequency/amount) · Tobacco/nicotine · Recreational or non-prescribed substances · Caffeine · Concerns about any of the above?
7. Social & Developmental History Living situation · Relationship/marital status · Children/dependents · Employment/education · Significant life events or trauma (only what you’re comfortable sharing now) · Cultural, religious, or spiritual factors relevant to your care · Support system
8. Goals for Treatment What would you like to be different? · How will you know therapy is working?
9. Administrative Insurance information · Preferred session format (in-person/telehealth) · Availability · How did you hear about us?
10. Consents (signature required) Informed consent for treatment · HIPAA privacy acknowledgment · Telehealth consent (if applicable) · Consent for AI-assisted documentation (if your practice uses it) · Cancellation/no-show policy
Keep a master copy and tailor per population, child/adolescent intake needs guardian sections and developmental history; couples intake needs each partner’s perspective.
What Each Section Captures — and Why
- Presenting concern anchors the clinical picture and starts your formulation. Open-ended phrasing surfaces more than checkboxes.
- Mental health and family history informs differential diagnosis and treatment planning before you’ve spent a session gathering it verbally.
- Risk screening is a flag, not an assessment. A “yes” tells you to conduct a proper clinical risk assessment in session, it never substitutes for one. (See our MSE cheat sheet for documenting risk findings.)
- Medical history and medications matter because physical conditions and drug interactions affect presentation and care coordination.
- Substance use is often under-reported; non-judgmental framing improves disclosure.
- Social/developmental history and cultural factors ground your understanding of the person, not just the symptom, and prevent misreading culturally normative behavior as clinical.
- Goals give you and the client a shared target and a measure of progress.
- Consents are the legal foundation; the AI-documentation consent line matters specifically if your practice uses AI tools.
Where AI Helps With Intake (and Where It Doesn’t)
Being candid about the boundary is what makes AI useful rather than risky.
Where AI genuinely helps:
- Summarizing a completed form into a one-minute clinical brief so you walk into the first session informed.
- Drafting the intake/biopsychosocial assessment note from the first session, the same way it drafts progress notes, structured, formatted, ready to edit.
- Reducing double entry by pushing intake data into your EHR rather than you re-typing it.
- Flagging items that warrant attention (e.g., a positive risk-screen response) for your review.
- Where a clinician decides:
- Clinical significance. AI can surface a reported symptom; only you decide what it means for diagnosis, risk, and treatment.
- Risk assessment. A form flag is not an assessment. The clinical risk evaluation and its documentation is yours.
- Rapport and nuance. The therapeutic relationship starts at intake; AI handles the paperwork so you can spend that first session connecting, not transcribing.
- Cultural interpretation. Whether a history detail is clinically relevant or culturally normative is a clinical judgment.
How AI Can Streamline Your Intake Workflow
Here’s how this fits together in practice, and where you stay in control.
Intake sits at the front of the practice workflow scheduling, onboarding, and the first clinical contact which is the domain of Supadesk on the Supahealth platform, while the intake assessment note is generated the same way Supanote drafts any clinical note: structured from the session, in your format, ready to edit and Super Fill into your EHR. [Confirm Supadesk page/URL before publishing.]
What AI handles for you: organizing intake responses into a usable summary, drafting the intake assessment note, reducing re-typing into the EHR, and flagging items for your attention.
Where you remain responsible: interpreting clinical significance, conducting and documenting the actual risk assessment, building rapport in the first session, and reviewing and signing the intake note. AI streamlines the administrative weight of intake so your clinical attention goes to the person in front of you it supplements the process, it doesn’t make clinical decisions.
If your interest is the platform side intake, scheduling, and onboarding workflows for a practice that’s a Supahealth conversation; book a live demo to see how it fits your operations. If your interest is specifically generating the intake assessment note from sessions, that’s Supanote, and you can try it for free.
Compliance and Consent
Intake forms collect the most sensitive PHI you hold risk history, substance use, trauma. Handling it demands the same rigor as any clinical data:
Use HIPAA-compliant forms and storage; confirm a BAA with any vendor that processes intake data.
Encrypt data in transit and at rest.
For AI tools, confirm your data isn’t used to train models and that recordings/inputs are minimized and deleted appropriately.
Include an explicit AI-documentation consent line if you use AI to draft intake notes, and check what your jurisdiction and ethics code require for disclosure.
(Our HIPAA-compliant AI apps guide has the full vendor checklist.)
Common Intake Pitfalls — Do/Don’t
- Don’t treat a positive risk-screen checkbox as an assessment. Do conduct and document a clinical risk assessment in session.
- Don’t use closed checkboxes for the presenting concern. Do ask open-ended questions that surface what a checkbox misses.
- Don’t skip the cultural/spiritual section. Do include it to avoid misreading normative behavior as pathology.
- Don’t collect sensitive PHI on a non-compliant form. Do use HIPAA-compliant intake with a BAA in place.
- Don’t omit AI-documentation consent if you use AI tools. Do make disclosure part of informed consent.
FAQ
Ques: Can AI conduct the intake assessment for me?
Ans: No, and you wouldn’t want it to. AI can summarize a completed intake form, draft the intake assessment note from your first session, and reduce data re-entry, but the assessment itself interpreting history, evaluating risk, forming a clinical impression, is yours. The right framing is that AI removes the transcription and formatting burden so you can spend the first session doing the clinical work.
Ques: Is it safe to collect intake information through an AI-powered form?
Ans: It’s safe if the tool is HIPAA compliant: a signed BAA, encryption in transit and at rest, clear data handling, and critically no use of your data to train models. Intake collects exceptionally sensitive PHI, so don’t use a general-purpose form builder that won’t sign a BAA. Verify compliance the same way you would for any clinical tool.
Ques: How is an AI intake summary different from just reading the form?
Ans: It saves time and surfaces structure. Instead of reading a long, sometimes disorganized completed form, you get a concise clinical brief that organizes the presenting concern, history, risk flags, and goals. You still read the underlying responses where it matters especially risk items but the summary lets you walk into the first session oriented rather than scrambling.
Ques: Does the risk-screening section replace a clinical risk assessment?
Ans: Absolutely not, and this is the most important thing to get right. The screening section is a flag a “yes” tells you to conduct a proper clinical risk assessment in the session. It never substitutes for clinical judgment, documentation, or a safety plan. Treat form responses as the prompt for assessment, not the assessment itself.
Ques: What should a mental health intake form include?
Ans: At minimum: identifying information, presenting concern, mental health history, risk screening, medical history and medications, substance use, social/developmental history with cultural factors, treatment goals, administrative/insurance details, and required consents. Tailor it to your population child intake needs guardian and developmental sections; couples intake needs each partner’s perspective. The template above is a complete starting point.
Ques: Do I need a separate consent for AI-assisted documentation?
Ans: Many practices include an explicit AI-documentation consent line, and depending on your jurisdiction and ethics code it may be required or strongly advisable. Even where it isn’t strictly mandated, disclosing that AI assists with notes is good practice and builds trust. Build it into your informed-consent process and document it.
Ques: Can AI handle intake for child or adolescent clients?
Ans: The drafting and summarizing functions work the same way, but the form needs developmental history and guardian sections, and consent involves the guardian. Clinically, intake with minors requires developmentally appropriate interpretation that’s entirely yours. AI handles the administrative structure; the clinical work with a young client is unchanged.
Ques: Will AI intake tools integrate with my EHR?
Ans: Good ones reduce double entry by pushing intake data and the drafted intake note into your existing EHR rather than creating a separate record. Confirm integration with your specific system before adopting, and prefer tools that sync into your chart so you’re not maintaining a second store of sensitive PHI.
Ques: How does AI intake handle telehealth clients?
Ans: Smoothly digital intake forms and AI summaries are format-agnostic, and telehealth clients complete the same online intake before the first session. Make sure your form includes telehealth consent and captures client location, and that the assessment note documents the telehealth-specific elements your payer requires.
Ques: What happens to the intake data the AI processes?
Ans: It depends on the vendor, so confirm before adopting. Privacy-first tools encrypt data, minimize what they retain, strip identifiers, and don’t train models on it. Given how sensitive intake data is, ask specifically about retention and deletion, and require a BAA. If a vendor is vague about data handling, don’t route intake PHI through it.
References
American Psychological Association. (2007). Record Keeping Guidelines. https://www.apa.org/practice/guidelines/record-keeping
American Psychiatric Association. (2016). Practice Guidelines for the Psychiatric Evaluation of Adults (3rd ed.). https://psychiatryonline.org/doi/book/10.1176/appi.books.9780890426760
U.S. Department of Health & Human Services. HIPAA Privacy Rule. https://www.hhs.gov/hipaa/for-professionals/privacy/index.html
U.S. Department of Health & Human Services. Business Associate Contracts. https://www.hhs.gov/hipaa/for-professionals/covered-entities/sample-business-associate-agreement-provisions/index.html
Substance Abuse and Mental Health Services Administration. SAFE-T: Suicide Assessment Five-Step Evaluation and Triage. https://store.samhsa.gov/product/safe-t-pocket-card-suicide-assessment-five-step-evaluation-and-triage-clinicians/sma09-4432
This article is educational and not legal advice. For consent and compliance decisions specific to your practice, consult a qualified healthcare attorney.
Written by Sam T, Founder & CEO of Supanote. Sam writes about behavioral health documentation, care workflows, and the operational realities of
