You have likely witnessed this scene countless times: a client sits across from you, reluctantly describing their drinking patterns. The details emerge gradually – blackouts they don’t fully remember, conflicts with loved ones, failed attempts to cut back, and the growing anxiety that accompanies their relationship with alcohol.
As you listen, your mind is already navigating the complex terrain of the ICD-10 codes for chronic alcohol use disorder, preparing to translate this human experience into the standardized language required for diagnosis and treatment planning.
Understanding Alcohol Use Disorder in ICD-10: The Essentials
The ICD-10-CM places alcohol-related disorders primarily under the F10 category within the broader “Mental, Behavioral and Neurodevelopmental Disorders” section.
Unlike the DSM-5’s dimensional approach, the ICD-10 separates alcohol dependence (F10.2x) from harmful use of alcohol (F10.1x), offering distinct diagnostic pathways that often require careful clinical judgment. “The correct ICD-10-CM code must reflect the specific clinical presentation. The ICD-10-CM Diagnosis Code for alcohol dependence is F10.20.
Accurate diagnosis is crucial as these disorders must be classified based on the substance most responsible for the patient's clinical presentation, and additional diagnoses should be coded when multiple substances are involved.
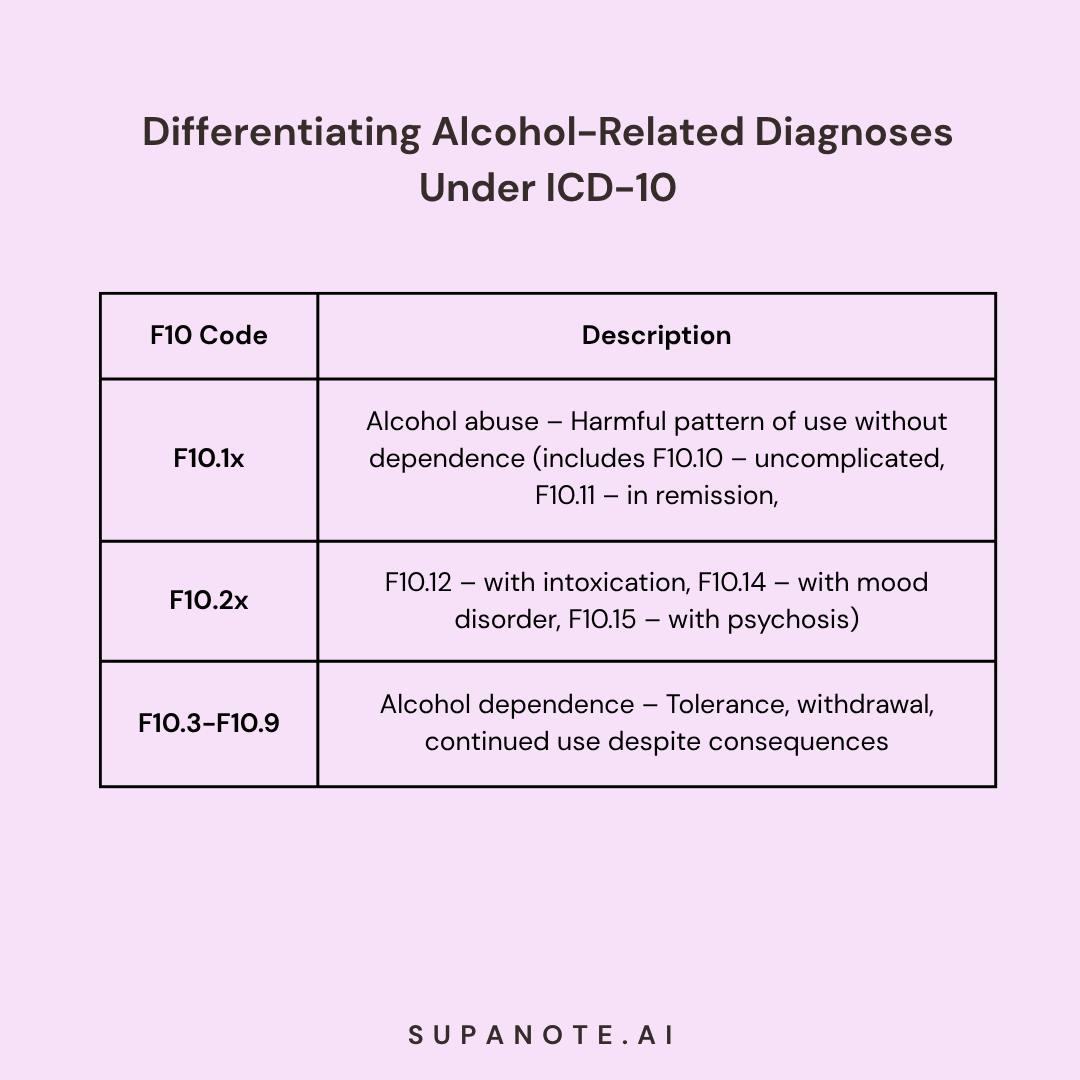
The F10 classification provides a comprehensive framework for documenting the spectrum of alcohol-related presentations:
- F10.1x - Harmful use of alcohol: Characterized by a harmful pattern of alcohol use without meeting criteria for dependence
- F10.2x - Alcohol dependence: Featuring tolerance, withdrawal, and continued use despite negative consequences. F10.20 is classified as uncomplicated alcohol dependence.
- F10.3-F10.9 - Alcohol-induced disorders: Covering various complications including withdrawal states, psychotic disorders, and persisting cognitive impairments
Each category requires additional characters to specify clinical details such as remission status, presence of perceptual disturbances, or complicating factors.
Clinical Assessment: Translating Client Experiences into ICD-10 Language
When evaluating a client for alcohol use disorder, the ICD-10 framework requires attention to several key aspects:
Pattern and frequency: The ICD-10 distinguishes between continuous use, episodic use (e.g., binge drinking), and other patterns that may influence coding decisions. Document not just how much, but how often and in what pattern your client consumes alcohol.
Physiological dependence: Evidence of tolerance and withdrawal symptoms strongly suggests alcohol dependence (F10.2x) rather than abuse (F10.1x). Listen for descriptions of needing increased amounts to achieve effects or experiencing discomfort when cutting back.
Behavioral indicators: The ICD-10 emphasizes behavioral aspects like compulsive use, continued consumption despite negative consequences, and prioritizing alcohol over other activities. These elements help differentiate between harmful use of alcohol and dependence.
Comorbid conditions: Be attentive to symptoms that might indicate alcohol-induced disorders such as psychosis (F10.5x), mood disturbances (F10.8), or cognitive impairments (F10.6), which require additional coding.
Understanding the etiology of alcohol use disorder is crucial for effective treatment. Identifying the underlying causes, including organic factors, can help in addressing the root issues and managing withdrawal states or related complications.
When documenting, remember the ICD-10’s emphasis on specificity. Unspecified alcohol abuse (F10.9) should be a temporary placeholder only when information is genuinely insufficient for a more precise diagnosis.
Have your clinical documentation done for free!
Try Now!
ICD-10 Coding in Practice: Common Clinical Scenarios
Scenario 1: Alcohol Dependence with Withdrawal
A 42-year-old client presents with increasing alcohol consumption over the past year, morning drinking to alleviate tremors, and failed attempts to cut back. During your assessment, they describe sweating, insomnia, and anxiety when attempting to reduce intake.
Appropriate coding: F10.239 (Alcohol dependence with withdrawal, unspecified)
If the client is experiencing hallucinations with delirium, use F10.231 instead, denoting withdrawal with perceptual disturbances.
Scenario 2: Alcohol Abuse with Intoxication
A 28-year-old client reports weekend binge drinking resulting in blackouts and risky behavior. They maintain normal functioning during weekdays with no daily drinking or withdrawal symptoms. They recently received a DUI charge following an episode of intoxication.
Appropriate coding: F10.129 (Harmful use of alcohol with intoxication, unspecified)
If their intoxication included perceptual disturbances, you would code F10.122 instead.
Scenario 3: Alcohol-Induced Disorders
A 56-year-old client with a 20-year history of heavy drinking presents with persistent memory problems, difficulty concentrating, and personality changes that remain even during periods of sobriety, highlighting the role of alcohol as a psychoactive substance in these disorders.
Primary code: F10.26 (Alcohol dependence with alcohol-induced persisting amnestic disorder)
You might also consider F10.27 (Alcohol dependence with alcohol-induced persisting dementia) depending on the severity and nature of cognitive impairment.
Beyond F10: Related Codes Therapists Should Know
While the F10 series forms the cornerstone of alcohol-related diagnoses, several other ICD-10 codes may prove relevant in your clinical work. Accurately identifying and coding diseases is crucial for effective health information management. Here are some important codes to consider:
- G31.2: Degeneration of nervous system due to alcohol
- K70.x: Alcoholic liver disease, including alcoholic hepatitis and cirrhosis
- Z71.41: Alcohol abuse counseling and surveillance of alcoholic
- O99.31x: Alcohol use complicating pregnancy, childbirth, and the puerperium
- Y90.x: Evidence of alcohol involvement determined by blood alcohol level. T51.x codes may be used in cases of toxic effect of alcohol when poisoning or overdose occurs.
For complex cases, consider using multiple codes to capture the full clinical picture. This may include coding opioid abuse (F11.10) if clients also misuse prescription painkillers. For instance, a client with alcohol dependence who develops alcoholic cirrhosis might be coded with both F10.20 and K70.30.
Diagnostic Challenges and Clinical Considerations
Differential Diagnosis
Several conditions may present similarly to alcohol use disorder or commonly co-occur, requiring careful assessment:
- Other substance use disorders: Polysubstance use is common and requires additional codes (F11-F19). For example, psychoactive substance dependence is often coded under F19.20 when alcohol is used alongside other drugs. The ICD-10-CM Diagnosis Code F19 is used for mental and behavioral disorders due to poly-substance use. It is crucial to distinguish between alcohol use disorder and other substance abuse issues. In milder cases, psychoactive substance abuse codes may be appropriate when dependence criteria are not met.
- Mood disorders: Distinguish between primary mood disorders and alcohol-induced mood disorders (F10.8)
- Anxiety disorders: Separate primary anxiety from alcohol-induced anxiety disorder (F10.980)
- Psychotic disorders: Differentiate between primary psychotic disorders and alcohol-induced psychotic disorder (F10.5x)
Cultural and Contextual Factors
The ICD-10, like all diagnostic systems, exists within cultural contexts that influence how symptoms are expressed and interpreted. Consider:
- Cultural norms around drinking that may affect self-reporting
- Gender differences in alcohol use patterns and physiological effects
- Age-related factors that influence both presentation and prognosis
- Socioeconomic factors affecting access to treatment
Documentation Best Practices for Reimbursement and Treatment Planning
Clear documentation not only ensures appropriate reimbursement but also enhances communication with other providers and guides effective treatment planning:
- Be specific: Provide a thorough description and avoid unspecified codes (those ending in .9) whenever possible. Include the full code title (e.g., “Alcohol dependence with psychotic disorder”) in treatment notes when possible.
- Document evidence: Include specific symptoms that support your diagnostic code
- Note severity: Include qualitative and quantitative measures of severity
- Update regularly: Revise coding as the clinical picture evolves
Remember that many insurance providers, including Medicaid services, require specific documentation to support alcohol use disorder diagnoses, particularly for higher levels of care.
Treatment Implications of ICD-10 Coding
Your selection of ICD-10 codes directly influences treatment decisions:
- F10.2x (Dependence) often indicates need for medically supervised withdrawal management
- F10.14-F10.15 (Abuse with psychotic symptoms) may necessitate antipsychotic medications and closer monitoring
- F10.6 (Amnestic disorder) suggests need for cognitive rehabilitation approaches
- F10.7 (Dementia) may warrant safety assessments and caregiver support
The specific 4th, 5th, and 6th characters in your coding should align with your treatment plan components and inform level of care decisions.
FAQs About Alcohol Use Disorder ICD-10 Coding
Q: What’s the difference between “in remission” codes for alcohol abuse vs. dependence?
A: For both abuse (F10.11) and dependence (F10.21), the “in remission” specifier indicates the person no longer meets criteria for the active disorder but has a history of meeting them. However, the threshold for what constituted the original disorder differs, with dependence requiring evidence of physiological dependence that abuse does not.
Q: Can I code both alcohol abuse and dependence simultaneously?
A: No. In the ICD-10 hierarchy, alcohol dependence takes precedence over abuse. If a client meets criteria for dependence, only code the dependence.
Q: When should I use “alcohol use, unspecified” (F10.9) vs. more specific codes?
A: The unspecified code should only be used temporarily when you have clear evidence of problematic alcohol use but insufficient information to determine if it meets criteria for abuse or dependence. It’s generally preferable to gather additional information to use a more specific code.
Q: How do I code when a client has both alcohol withdrawal and alcohol-induced anxiety?
A: When multiple alcohol-induced conditions are present, you must prioritize. Withdrawal (F10.23x) generally takes precedence in coding over induced anxiety (F10.980) during acute presentation. You can document the anxiety symptoms in your notes even if they don’t appear in the primary code.
Q: How do blood alcohol levels relate to ICD-10 codes?
A: Blood alcohol levels (Y90.x codes) can be used as additional codes to provide objective evidence of intoxication, but they don’t replace clinical assessment for diagnosis of alcohol use disorders.
Q: How do I categorize mental and behavioral disorders when the specifics of substance use are unclear?
A: When the specifics of substance use are unclear, and multiple psychoactive substances are involved, the term 'unknown' is used. This applies when it is difficult to determine which substances are contributing to the disorders, often because users may not be aware of all the substances they are consuming.
Navigating the Spectrum of Other Alcohol-Induced Disorders
When working with clients who have alcohol-related issues, it's essential to recognize the full range of other alcohol-induced disorders that may be present. Beyond the commonly identified patterns of alcohol abuse and alcohol dependence, the ICD-10 provides specific codes for conditions that may emerge as consequences of alcohol use:
Alcohol-induced psychotic disorder (e.g., F10.151, F10.251, F10.951) presents with hallucinations, delusions, or both that develop during or shortly after alcohol intoxication or withdrawal. These symptoms are directly attributable to alcohol use and typically resolve within a short period following cessation, distinguishing them from primary psychotic disorders.
Note - Although the general category is referred to as F10.5 in some references, F10.5 alone is not a valid ICD-10-CM billing code. Clinicians must select the appropriate full code based on clinical context, whether the client meets criteria for alcohol abuse (F10.151), alcohol dependence (F10.251), or unspecified use (F10.951) with psychotic features.
Alcohol-induced sleep disorder (F10.982) encompasses insomnia, hypersomnia, or parasomnia directly resulting from alcohol consumption or withdrawal. Many clients fail to connect their sleep disturbances to their drinking patterns, making careful assessment critical.
Alcohol-induced sexual dysfunction (F10.981) includes difficulties with desire, arousal, or performance directly attributable to alcohol use. This often-overlooked consequence can significantly impact relationships and quality of life.
Unspecified alcohol-induced disorder (F10.99) serves as a diagnostic placeholder when a client clearly shows signs of an alcohol-induced condition that doesn't fit neatly into other categories. While using this code, continue gathering clinical data to refine the diagnosis when possible.
When documenting these conditions, remember that specificity improves both clinical communication and reimbursement outcomes. The phrase "unspecified alcohol-induced disorder" should be reserved for truly ambiguous presentations where additional assessment is pending.
Automating Therapy Documentation with AI
With the advancement of technology, mental health professionals are turning to AI Therapy Note tools like Supanote to automate their documentation. These tools -
- Automatically create nuanced clinical documentation
- Can automatically identify the ICD code for your session
- Prevent billing and coding errors
- Reduce time spent on paperwork, allowing more focus on patient care.
Proper documentation and coding are crucial for ensuring that services provided are eligible for Medicare reimbursement. Adhering to specific coding guidelines is essential for financial support from this government program.
For example, at the end of a session, Supanote would directly generate the relevant progress notes in your preferred format (SOAP, DAP, GIRP, etc.), along with a mental status examination, and relevant CPT and ICD codes.
Get your Personal AI Scribe
Let Supanote handle your clinical documentation while you focus on what matters most
Get It Now!
Resources for Therapists
Assessment Tools
- AUDIT (Alcohol Use Disorders Identification Test)
- CIWA-Ar (Clinical Institute Withdrawal Assessment for Alcohol, Revised)
- ASI (Addiction Severity Index)
Clinical References
- ASAM Criteria for Substance Use Treatment Placement
- WHO Guidelines for the Identification and Management of Substance Use Disorders
Patient Education Materials
As therapists, our success with clients struggling with alcohol use disorder depends not only on our clinical skills but also on our ability to navigate diagnostic systems accurately. By mastering the ICD-10 framework for alcohol-related disorders, we enhance our capacity to communicate effectively with other providers, secure appropriate reimbursement, and—most importantly—develop treatment plans that meaningfully address our clients' needs. The codes may seem like administrative requirements, but in skilled hands, they become powerful tools for translating complex human experiences into pathways toward healing.
